سندرم تخمدان پلی کیستیک (PCOS) یک بیماری شایع هورمونی است که در آن، به دلیل ترشح مقدار زیادی هورمون آندروژن، فرد دچار تخمکگذاری نامنظم و یا حتی عدم تخمکگذاری میشود. این عدم تخمکگذاری مشکلاتی را در زمینه باروری به وجود میآورد که پزشک معالج یکی از روشهای زیر را جهت رفع مشکلات باروری تجویز میکند:
- کلومیفن (Clomiphene): یکی از رایجترین داروها جهت درمان ناباروری ناشی از سندرم تخمدان پلی کیستیک (PCOS) و القای تخمکگذاری است. احتمال باردار شدن 2 قلو و یا 3 قلو در زنانی که از داروهای کلومیفن استفاده میکنند (از هر 10 نفر، 1 نفر) بیشتر از زنانی است که بهطور طبیعی باردار میشوند.
- متفورمین (Metformin): یکی از داروهای حساس کننده به انسولین است که معمولاً جهت درمان بیماری دیابت استفاده میشود و برای بیشتر زنان مبتلا به سندرم تخمدان پلی کیستیک به کار گرفته میشود. این دارو آثار مثبتی روی منظم سازی تخمکگذاری و یا افزایش تخمکگذاری داشته و گاهی اوقات در ترکیب با کلومیفن استفاده میگردد. تحقیقات نشان میدهد که متفورمین به تنهایی و یا در ترکیب با کلومیفن، در افزایش تخمکگذاری تأثیر به سزایی خواهد داشت، در صورتیکه در میزان بارداری تأثیر مستقیمی ندارد.
- لتروزول (Letrozole): این دارو تولید استروژن را کاهش داده و به اندازه تأثیر داروی کلومیفن در تنظیم بارداری، تخمکگذاری را تنظیم میکند و میزان بارداری را بهبود میبخشد. در حال حاضر، مرکز تحقیقات NICHD در حال انجام مطالعات در ارتباط با مقایسه تأثیر داروهای کلومیفن و لتروزول بر روی حیوانات است. اگر داروهای ذکر شده در میزان باروری شخص بیمار هیچ تأثیری نداشته باشند، پزشک معالج روشهای درمانی دیگری را تجویز میکند.
- گنادوتروپین (Gonadotropin): هورمونهایی هستند که موجب تنظیم تخمکگذاری میشوند. این روش درمانی پرهزینه بوده و در درمان بارداری نسبت به داروی کلومیفن ریسک بالاتری دارد. در این روش درمانی، انجام تستهای آزمایشگاهی و اولتراسوند جهت مشخص شدن میزان تأثیرگذاری روش درمانی نیاز است.
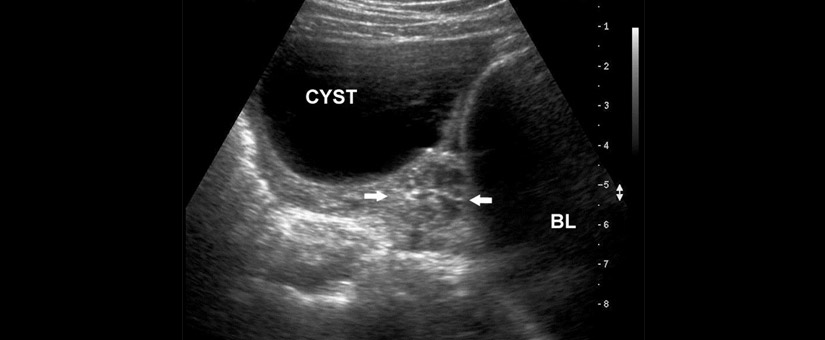
- لاپاراسکوپی: یک روش تشخیصی و درمانی ناباروری در بیماران مبتلا به سندرم کیست تخمدان است. در صورتیکه دارو هیچ تأثیری در تخمکگذاری و حاملگی نداشته باشد، جراحی لاپاراسکوپی تخمدان که بهصورت سرپایی انجام میشود توسط پزشک معالج تجویز خواهد شد. این جراحی احتمال تخمکگذاری را افزایش میدهد به خصوص اگر سطح آندروژن کمتر باشد. در این روش پزشک از طریق ایجاد برش کوچکی بر روی شکم (زیر ناف) یک لوله باریک دوربیندار (لاپاراسکوپ) و سایر وسایل مورد نیاز مثل گیره، قیچی و نخ بخیه را از طریق 2 یا 3 سوراخ به داخل شکم بیمار فرستاده و تخمدانها و رحم را مشاهده میکند. این دوربین تصاویری با جزئیات از تخمدانها در اختیار جراح قرار میدهد که در صورت مشاهده کیست تخمدان میتواند کیست را با استفاده از لاپاراسکوپ از داخل شکم تخلیه کند. این عمل جراحی از سایر روشهای درمانی از جمله درمان با گنادوتروپین کم هزینهتر است.
Polycystic Ovary Syndrome (PCOS) is a common hormonal condition in which women produce a surplus of androgens. This causes irregular ovulation or even a lack of ovulation. The problems with ovulation, women with PCOS may have difficulty becoming pregnant. If a person have PCOS-related infertility, it’s health care provider may prescribe one of the following medications to help it’s get pregnant:
- Clomiphene: This is the most common treatment for infertility in women with PCOS. The Clomiphene indirectly causes eggs to mature and be released. One in 10 Women treated with clomiphene are more likely to have twins or triplets than women who get pregnant naturally.
- Metformin: Although this insulin-sensitizing drug is normally used to treat diabetes, it may also be used as an adjunct to increase or regulate ovulation in women with PCOS. Metformin can be used alone or used with clomiphene when clomiphene alone is not successful. Evidence shows that metformin—both alone and in combination with clomiphene increases ovulation, but it does not increase the rate of pregnancy.
- Letrozole: This drug transiently slows estrogen production and causes the body to make more follicle-stimulating hormone (FSH), a hormone needed for ovulation. Letrozole is as effective as clomiphene in causing ovulation. Studies of letrozole in animals have shown that it causes birth defects if used during pregnancy, but there have been no studies of this drug in pregnant women. If person do not get pregnant with these first-line medications, his/her health care provider may suggest one of the following treatments:
- Gonadotropins: These hormones, given as shots, cause ovulation. This treatment is costly and has a higher risk of multiple pregnancies than does treatment with clomiphene. The health care provider may need to use frequent laboratory tests and ultrasound exams to watch how your body responds to this treatment.
- Laparoscopy: This surgery may increase the chance of ovulation. In ovarian drilling the surgeon makes a small cut in your abdomen and inserts a long, thin tool called a laparoscope.
The surgeon then uses a needle with electric current to puncture and destroy a small part of the ovary. During laparoscopy other necessary tools such as clamp, tissues, scissors and yarn stitch by 2 or 3 other hole that goes into the abdomen below the navel is created. The surgery leads to lower androgen levels, which may improve ovulation. This surgery may be less costly than treatment with gonadotropin, and it does not seem to increase the risk of multiple pregnancies.